Prostate Cancer: Radical Prostatectomy
Radical prostatectomy is surgery to remove the entire prostate gland, some surrounding tissue, and seminal vesicles. Sometimes the nearby lymph nodes are also removed. This surgery may be done if tests show that the cancer is only found in the prostate, you have a life expectancy of at least 10 years, and you're healthy enough to have surgery.
Your surgeon will give you detailed instructions on getting ready for surgery. After surgery, you’ll be told how to care for yourself at home as you recover. Ask any questions you have about the procedure and recovery. Also ask about possible side effects and what can be done to help prevent them or treat them.
Risks and possible complications
All surgeries have risks. The risks of this surgery include:
-
Blood clots in your legs or lungs
-
Excess bleeding
-
Damage to nearby tissues and organs
-
Hole (perforation) in the bowel (This is rare.)
-
Infection
-
Reactions to the medicines used to make you sleep during surgery (anesthesia)
Side effects of prostate surgery can include:
-
Loss of bladder control (incontinence)
-
Lung infection (pneumonia)
-
Trouble getting or keeping an erection (erectile dysfunction)
-
Trouble peeing
-
Infertility
-
Orgasm changes
-
Shorter penis
-
Long-term swelling in the legs or groin (lymphedema). (This is rare.)
-
Increased risk for hernia
Talk with your treatment team about the risks of surgery and what can be done about them. Be sure you know what to expect and what to watch for after surgery.
Getting ready for your surgery
Follow all instructions from your healthcare team. Here are some of the things you might be asked to do:
-
Tell your healthcare provider about all medicines you take. This includes all prescription and over-the-counter medicines as well as herbs, vitamins, and other supplements. It also includes CBD, marijuana, or illegal drugs. You may need to stop taking some or all of them before the surgery.
-
You may be told to use a laxative, enemas, or both before the surgery. This is to empty the colon and rectum of stool. Follow the instructions you are given.
-
Follow all directions you are given for not eating or drinking before surgery.
How the surgery is done
There are different ways to do prostate surgery and different ways to reach the prostate to do it. Your treatment team will talk with you about the plan they think is best for you.
The surgery may be done through many small cuts (incisions) made in the belly (abdomen). This is called minimally invasive laparoscopic surgery. Long, thin tools are put into these cuts to take out the prostate. One of these tools has a light and video camera on the end that allows the surgeon to see inside your body. A method called robotic-assisted laparoscopy is often used. This system uses robotic arms that the surgeon controls to do the surgery with more precision. It also gives a close-up 3-D view inside the body.
Sometimes an open prostatectomy is done. This means the surgery is done through a large cut (incision) made on your skin. When the cut is in the lower belly, it's called the retropubic approach. In some cases, the surgery might be done through an incision behind your scrotum. This is called the perineal approach. It's not used as often.
During the surgery:
-
The surgeon may remove and test lymph nodes near the prostate. This is to see if cancer has spread to them. If it has, the surgeon may decide not to remove the prostate. That's because it isn't likely that the cancer could be cured with surgery. And removing the prostate can cause side effects.
-
The prostate, seminal vesicles, and part of the urethra will be taken out.
-
Nerve-sparing methods may be used to try to save erectile function.
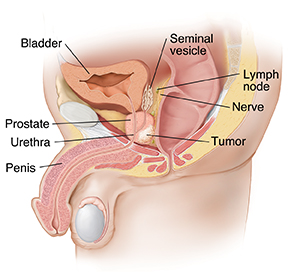 |
| The prostate, the seminal vesicles, and a portion of the urethra are removed. |
After surgery
A Foley catheter will be put through your penis and into your bladder during the surgery. It's used to drain urine from your bladder into a bag. Your urine may be bloody or cloudy at first. This is normal. The Foley catheter will stay in for a few weeks while you heal.
Recovering at home
You may go home 1 to 3 days after surgery. The Foley catheter will be left in. You'll be taught how to manage it at home.
You’ll be given medicines to control pain. Your healthcare team will teach you how and when to use your pain medicines. They will also:
-
Show you how to take care of your incision
-
Tell you what activities you can and can't do
-
Let you know when you can drive and when you can go back to work
-
Tell you when you should call them with concerns
-
Schedule your next appointment
Plan to give yourself time to rest and heal for the first few weeks.
Follow-up care
The Foley catheter and stitches will be removed at a follow-up visit. This is often 1 to 2 weeks after surgery. Bladder control often takes a few weeks to several months to return. It can continue to get better for up to 1 year.
When to call your healthcare provider
Call your provider right away if you have any of these:
-
Chills
-
Fever of 100.4°F (38°C) or higher, or as advised by your provider
-
Fluid leaking from your incision
-
Redness, swelling, or pain at the incision site that gets worse
-
Your incision opens
-
New swelling in your groin or leg
-
Pain that's not controlled or is getting worse
-
Swelling, warmth, redness, or pain in your leg
-
Trouble moving your bowels
-
Shortness of breath
-
Urine not draining from the catheter
-
Trouble peeing after the catheter has been removed
Be sure you know what other problems you should watch for. Also know how to get help any time, including after office hours, on weekends, and on holidays.